
| Quick Answer: What Is an Ear Infection?An ear infection (otitis media) occurs when bacteria or viruses infect the fluid trapped behind the eardrum. The most common ear infection symptoms include sharp ear pain, a feeling of fullness in the ear, muffled hearing, and fever. Most mild infections clear up within 2–3 days. Bacterial cases are treated with antibiotics; viral cases require symptom management and rest. Ear infections themselves are not contagious, but the viruses that trigger them are. |
Ear infections are among the most common — and most painful — health conditions in the world. By the time a child reaches age three, most will have experienced at least one. Adults are not spared either. Whether you are woken at 2 a.m. by severe ear pain, watching your infant tug at their ear in distress, or trying to figure out how to alleviate ear infection pain without a prescription, this guide has every answer you need.
WHAT YOU WILL LEARN:
Types of ear infections · Ear infection symptoms in children vs. adults · What an ear infection looks like · What causes ear infections · Are ear infections contagious? · How to treat an ear infection · How to alleviate ear infection pain at home · When to see a doctor · Prevention · FAQs
What Is an Ear Infection?
An ear infection — formally called acute otitis media — is an inflammatory condition in which bacteria or viruses multiply in fluid trapped inside the middle ear, the hollow space directly behind the eardrum. The eustachian tubes, which run from the middle ear to the back of the throat, normally drain this fluid and regulate pressure. When those tubes become swollen or blocked — most often due to a cold, flu, sinus infection, or allergy — fluid pools and creates the perfect environment for infection to take hold.
The infection causes the eardrum to become inflamed and sometimes to bulge outward, producing the hallmark symptom: ear pain. In more serious cases, pressure builds until the eardrum ruptures, releasing pus or bloody fluid. While that sounds alarming, a ruptured eardrum usually heals on its own within a few weeks.
3 Types of Ear Infections You Should Know
Understanding which type of ear infection is present matters — it influences the correct treatment approach.
| Type | Location Affected | Primary Cause | Who Gets It Most | Key Symptom |
| Middle Ear (Otitis Media) | Behind the eardrum | Bacteria or virus | Children 6 mo – 2 yrs | Ear pain, fever, fluid drainage |
| Outer Ear (Swimmer’s Ear / Otitis Externa) | Ear canal | Bacteria (water exposure) | Swimmers, all ages | Pain when outer ear is touched |
| Inner Ear (Labyrinthitis) | Inner ear structures | Virus (rare: bacteria) | Adults, any age | Dizziness, nausea, hearing loss |
Middle Ear Infection (Most Common)
This is the ear infection most parents and patients know. Bacteria or viruses infect stagnant fluid behind the eardrum. The AAP estimates middle ear infections account for roughly 30 million doctor visits in the United States each year. Children are most vulnerable due to the anatomy of their shorter, more horizontal eustachian tubes.
Outer Ear Infection — Swimmer’s Ear
Swimmer’s ear affects the ear canal itself. Prolonged water exposure strips the canal’s protective acidic coating, allowing bacteria to colonize. It is identified by pain or tenderness when the external ear is pulled or pressed — a distinguishing feature that sets it apart from middle ear infections. Treatment focuses on antibiotic ear drops, not oral antibiotics.
Inner Ear Infection
The least common but most debilitating type. Inner ear infections cause inflammation of the labyrinth (labyrinthitis) or vestibular nerve (vestibular neuritis), resulting in severe dizziness, balance disturbances, nausea, and in some cases temporary hearing loss. They are almost always viral and require rest and symptom management rather than antibiotics.
Ear Infection Symptoms: A Complete Breakdown by Age
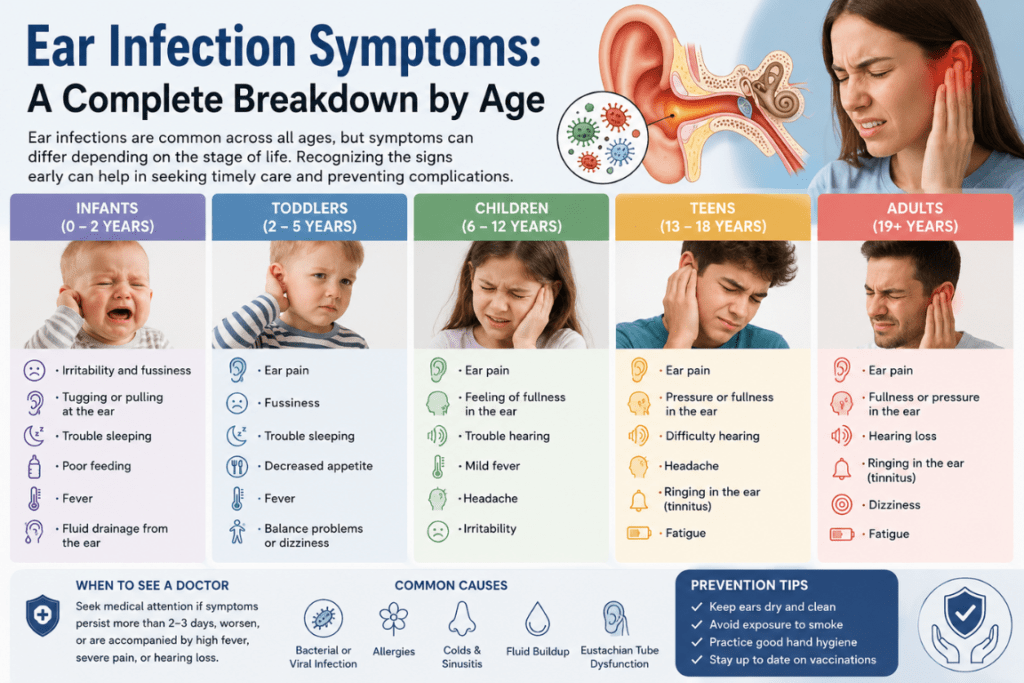
Recognizing ear infection symptoms early prevents the condition from worsening. A critical point: symptoms differ significantly between infants, older children, and adults. Here is exactly what to look for at each stage.
| How do you know if you have an ear infection?The most reliable ear infection symptoms are: (1) ear pain or pressure, especially when lying down; (2) muffled or reduced hearing; (3) fever; (4) fluid or pus draining from the ear. In infants, watch for tugging at the ear, unusual crying, and difficulty feeding. In adults, dizziness and balance problems may also appear. A confirmed diagnosis requires a doctor to examine the eardrum with an otoscope. |
Ear Infection Symptoms in Infants and Toddlers
Young children cannot tell you their ear hurts. They communicate through behavior. Key warning signs include:
• Persistent tugging, pulling, or batting at one or both ears
• Inconsolable crying, unusual irritability, or fussiness that seems unexplained
• Refusing the bottle or breast — swallowing changes middle ear pressure, intensifying pain
• Disrupted sleep; waking more than usual during the night
• Fever of 100°F (38°C) or higher
• Fluid — clear, yellow, or blood-tinged — draining from the ear
• Failure to respond normally to sounds or voices
• Loss of balance, stumbling, or general unsteadiness
Ear Infection Symptoms in Older Children and Adults
Once a child can describe what they feel, the picture becomes clearer. Adults typically present with:
• Sharp, stabbing, or dull throbbing ear pain — often described as severe ear pain that worsens at night
• A sensation of fullness, pressure, or “blockage” in the affected ear
• Muffled hearing or a temporary drop in hearing ability
• Fever, fatigue, and general feeling of being unwell
• Fluid or pus draining from the ear canal
• Dizziness or vertigo (especially with inner ear involvement)
• Headache and neck stiffness in severe cases
• Ear discomfort during a cold — a very common early warning that the infection is developing
Important: Severe ear pain that suddenly disappears may signal a ruptured eardrum — do not interpret this relief as recovery. See a doctor immediately for evaluation.
What Does an Ear Infection Look Like?
This is one of the most searched questions related to ear infections — and understandably so. The answer is that you cannot see an ear infection from the outside with the naked eye. The changes happen inside the ear canal and behind the eardrum, which is why a proper diagnosis always requires an otoscope.
What a Healthy Eardrum Looks Like
A normal eardrum (tympanic membrane) is translucent or pearly gray, cone-shaped, and reflects light cleanly. It sits taut and flat and moves freely when air is blown against it with a pneumatic otoscope.
What an Infected Eardrum Looks Like
When infection is present, the eardrum undergoes visible changes that a trained clinician can identify immediately:
• Color shift: The membrane turns red, orange, or deep pink — indicating inflammation
• Bulging: Pus and fluid accumulating behind the eardrum push it outward, giving it a domed appearance
• Opacity: The normally translucent membrane becomes cloudy or white, obscuring the middle ear structures
• Reduced mobility: On pneumatic otoscopy, the eardrum moves poorly or not at all due to fluid behind it
• Fluid level: In some cases, a visible line (air-fluid interface) can be seen behind the membrane
• Perforation: If the eardrum has ruptured, a tear is visible with fluid actively draining through it
External Signs You Can See
While the eardrum itself is not visible without instruments, a few external clues may suggest an infection is present:
• Redness or swelling around the outer ear opening
• Visible fluid or discharge (pus, clear liquid, or blood) draining from the ear canal
• Swelling or tenderness of the lymph nodes just below or behind the ear
• In swimmer’s ear, the outer ear may appear swollen and the ear canal visibly narrowed
What Causes Ear Infections? 7 Root Causes Explained
Ear infections rarely appear out of nowhere. They are almost always the downstream consequence of another condition that impairs eustachian tube function or introduces bacteria and viruses into the middle ear.
1. Common Colds and Upper Respiratory Infections
The common cold is the single leading cause of middle ear infections. Cold viruses cause nasal congestion and swelling that spreads to the eustachian tubes. Once those tubes are blocked, fluid accumulates and stagnates — and within 24 to 72 hours, a secondary bacterial infection may develop. This is why ear discomfort during a cold is such a reliable early warning sign that an ear infection may be on the way.
2. Bacterial Pathogens
Three bacteria are responsible for the vast majority of bacterial ear infections: Streptococcus pneumoniae (the most common), Haemophilus influenzae, and Moraxella catarrhalis. These organisms flourish in the warm, fluid-filled middle ear space created when eustachian tube drainage fails.
3. Viral Infections
Roughly 25 to 40 percent of ear infections are caused directly by viruses — including rhinovirus, respiratory syncytial virus (RSV), influenza, and adenovirus. Viral ear infections do not respond to antibiotics, which is why watchful waiting is often the recommended approach for mild cases.
4. Allergies
Seasonal allergies, food sensitivities, and environmental allergens trigger nasal inflammation that can chronically obstruct the eustachian tubes. Children with untreated allergies are significantly more prone to recurrent ear infections. Managing the underlying allergy often reduces the frequency of infections dramatically.
5. Anatomical Factors — Why Children Are More Susceptible
Children’s eustachian tubes are shorter, narrower, and lie at a more horizontal angle than those of adults. This means fluid drains less efficiently and bacteria can more easily travel from the throat to the middle ear. Children’s immune systems are also still developing, offering less defense against new pathogens. By contrast, adult eustachian tubes are longer and angled downward, allowing better drainage.
6. Environmental and Behavioral Risk Factors
A range of modifiable factors significantly elevate risk:
• Secondhand tobacco smoke — irritates and inflames eustachian tube lining, impairing its function
• Group childcare settings — rapid pathogen circulation between children
• Bottle-feeding while lying flat — allows milk to pool at eustachian tube openings
• Prolonged pacifier use after 6 months of age
• Swimming or water sports — increases risk of outer ear infection (swimmer’s ear)
• Inserting cotton swabs or objects into the ear canal — disrupts the protective wax barrier
7. Compromised Immune System
Any condition that weakens immune defenses — including diabetes, HIV/AIDS, autoimmune disorders, or immunosuppressive medications — dramatically increases susceptibility to ear infections, and can make infections harder to clear without medical intervention.
Are Ear Infections Contagious? The Research-Backed Answer
| Is an ear infection contagious?No. Ear infections themselves are not contagious — you cannot “catch” one from another person. However, the viruses and bacteria that trigger ear infections (such as cold and flu viruses) are highly contagious and spread through respiratory droplets and surface contact. This is why ear infections cluster in settings like daycares and schools: children pass the cold virus to each other, and some develop ear infections as a secondary complication. |
The nuance here is important for parents. If your child has an ear infection with no fever and is otherwise acting normally, they can usually attend school or daycare. However, if they are unwell — running a fever, clearly uncomfortable — keeping them home protects classmates from the underlying cold or flu virus, not from the ear infection itself.
Bacterial ear infections have a slightly different dynamic. While the infection itself is still not directly transmissible ear-to-ear, certain bacteria such as Streptococcus pneumoniae can spread between children in close contact. Vaccination against these bacteria (via the pneumococcal vaccine) remains the best structural defense.
How Is an Ear Infection Diagnosed?
A correct diagnosis is essential before beginning any ear infection treatment — particularly before deciding whether antibiotics are needed. Here is what to expect at a medical appointment:
1. Medical history review — the provider will ask about recent illness, symptom duration, and prior ear infections
2. Otoscope examination — a lighted, magnifying instrument used to visualize the ear canal and eardrum
3. Pneumatic otoscopy — a puff of air tests eardrum mobility; a non-moving drum suggests fluid accumulation
4. Tympanometry — a probe measures middle ear pressure and the eardrum’s acoustic response
5. Hearing evaluation — ordered for children with chronic or recurring infections to check for hearing impact
6. Ear fluid culture — sometimes performed by specialist if infection is severe, recurrent, or not responding to treatment
Telemedicine note: Some pediatric telehealth platforms now provide video otoscopes that parents use at home to capture live footage of the eardrum, which a board-certified physician reviews remotely. This is a growing option for initial evaluation, especially in rural areas.
Ear Infection Treatment: What Works and When
The right ear infection treatment depends on the patient’s age, the severity and duration of symptoms, whether the infection is viral or bacterial, and whether antibiotics are likely to add value. Here is a structured guide to the full treatment spectrum:
Option 1: Watchful Waiting (Active Observation)
Not every ear infection requires medication. The American Academy of Pediatrics (AAP) endorses a watchful waiting period of 48–72 hours for children aged 2 and older with mild symptoms, non-severe pain, and no fever above 102.2°F (39°C). During this window, the immune system often clears the infection on its own — and this approach avoids the antibiotic overuse that drives resistance.
Watchful waiting is not passive. Parents should monitor for worsening symptoms and use pain management (see below) throughout the observation period.
Option 2: Antibiotics — When They Are and Are Not Appropriate
Antibiotics are the definitive ear infection treatment for confirmed bacterial infections or when:
• The child is under 2 years of age
• Both ears are infected simultaneously
• Symptoms are severe — fever above 102.2°F or intense pain
• Symptoms do not improve or worsen after 48–72 hours of watchful waiting
• The patient has a cochlear implant, cleft palate, or immune deficiency
Amoxicillin is the first-line antibiotic of choice. For penicillin-allergic patients, cephalosporins or azithromycin are alternatives. The full course — typically 7–10 days — must be completed even if symptoms resolve earlier. Stopping early risks relapse and contributes to antibiotic resistance.
Critical: Antibiotics do not work against viral ear infections. Prescribing them inappropriately accelerates the development of drug-resistant bacteria.
Option 3: Ear Drops
For outer ear infections (swimmer’s ear), antibiotic ear drops — such as ciprofloxacin-hydrocortisone — are the preferred treatment. They deliver medication directly to the site of infection with minimal systemic side effects. Ear drops are not appropriate if the eardrum is perforated or if there is any possibility of a ruptured eardrum without medical confirmation.
Option 4: Pain and Fever Management
Over-the-counter pain relievers — ibuprofen (Advil, Motrin) or acetaminophen (Tylenol) — are safe and effective for managing ear infection pain and associated fever in both children and adults. Ibuprofen is generally preferred for pain above 6 months of age due to its dual anti-inflammatory effect. Never give aspirin to children due to the risk of Reye’s syndrome.
Option 5: Ear Tubes (Tympanostomy)
Surgical ear tube insertion is recommended for children who experience:
• Four or more ear infections within one year
• Three or more infections within six months
• Persistent fluid in the middle ear lasting more than three months with associated hearing loss
The procedure takes 10–15 minutes under general anesthesia. A tiny plastic or metal tube (grommet) is placed through a small incision in the eardrum, allowing fluid to drain continuously and equalizing pressure. Tubes remain in place 6–18 months and typically fall out on their own. Hearing often improves immediately after the procedure.
How to Alleviate Ear Infection Pain: 8 Home Remedies That Actually Work
While medical treatment addresses the underlying infection, home strategies can meaningfully reduce ear pain, pressure, and discomfort — especially during the watchful waiting period or while waiting for antibiotics to take effect. Here is how to get rid of ear infection discomfort using safe, evidence-supported approaches:
1. Warm or Cold Compress
A warm, damp washcloth held against the outside of the ear for 15–20 minutes relaxes tense muscles around the ear canal, encourages eustachian tube drainage, and provides genuine pain relief. If warmth does not help, try a cold pack wrapped in a cloth — cold reduces inflammation and numbs pain. Some people find alternating between warm and cold every 10–15 minutes works best.
2. OTC Pain Relievers — First-Line Home Treatment
Ibuprofen or acetaminophen remain the most reliable and fastest-acting home treatment for ear pain. They take effect within 30–60 minutes and are safe for most ages when dosed correctly. Check weight-based dosing charts for children. Prescription-strength ibuprofen doses can be discussed with your pharmacist.
3. Elevated Head Position
Lying completely flat increases middle ear pressure. Sleeping with the head elevated on two or more pillows — or propping an infant at a slight incline — reduces pressure inside the ear and allows gravity to assist fluid drainage. Many patients report significant overnight improvement using this simple strategy.
4. Hydration and Warm Fluids
Drinking plenty of fluids thins mucus secretions and keeps the nasal passages and eustachian tube lining moist and functional. Warm liquids — herbal tea with honey, clear broth, or warm lemon water — can help loosen congestion that is contributing to eustachian tube blockage. Managing ear discomfort during a cold is often about managing the cold itself first.
5. Humidifier and Steam Inhalation
Running a cool-mist humidifier in the bedroom adds moisture to the air, soothing inflamed nasal passages and reducing congestion. Brief steam inhalation — leaning over a bowl of hot water with a towel draped over the head — can temporarily open eustachian tubes and relieve the sensation of fullness. Do not use steam for infants or very young children due to burn risk.
6. Gentle Neck and Jaw Movements
Muscle tension around the ear canal amplifies pain. Gentle exercises help: slowly rotate the head in wide circles, tilt each ear toward the shoulder and hold for five seconds, open the jaw as wide as comfortable, or chew gum. These movements activate muscles that open the eustachian tubes, potentially helping trapped fluid shift and drain.
7. Diluted Hydrogen Peroxide Drops
A diluted solution (equal parts 3% hydrogen peroxide and clean water) can help clear earwax buildup that may be worsening ear discomfort. Place 2–3 drops in the affected ear, allow the bubbling to work for one minute, then drain. Use this method only for outer ear issues and only when the eardrum is known to be intact — never use it if you suspect a perforated eardrum or have ear tubes.
8. Garlic or Ginger (Topical, Not Internal)
Both garlic and ginger contain natural antimicrobial and anti-inflammatory compounds (allicin and gingerols, respectively). Applying a few drops of garlic-infused olive oil or fresh ginger juice around — not inside — the outer ear canal may provide mild anti-inflammatory relief. This is a supportive measure, not a substitute for medical treatment. Always consult a doctor before using any plant-based remedy on infants.
What NOT to do: Never insert cotton swabs, fingers, candles, or any object into the ear canal. This pushes infected material deeper, risks puncturing the eardrum, and almost always worsens the condition.
When to See a Doctor: Red Flag Symptoms
Home care is appropriate for mild-to-moderate symptoms when the patient is otherwise well. However, the following signs require prompt medical evaluation — waiting risks serious complications:
| Warning Sign | What It May Indicate | Action |
| Severe ear pain lasting more than 48–72 hours | Bacterial infection requiring antibiotics | See doctor within 24 hours |
| Sudden cessation of pain after intense discomfort | Possible ruptured eardrum | See doctor same day |
| Pus, blood, or cloudy fluid draining from ear | Perforated eardrum or severe infection | See doctor same day |
| Fever above 102.2°F (39°C) in child | Systemic spread of infection | Seek care promptly |
| Any fever in infant under 3 months | High-risk population | Emergency care |
| Swelling or redness behind the ear | Possible mastoiditis | Emergency care |
| Dizziness, severe headache, or facial weakness | Possible inner ear or neurological spread | Emergency care |
| Hearing loss that does not improve after infection resolves | Fluid in middle ear or nerve damage | ENT referral |
| 4+ ear infections in 12 months | Chronic otitis media — surgical evaluation | ENT consultation |
Untreated ear infections can lead to: permanent hearing loss, ruptured eardrum, mastoiditis (bone infection behind the ear), labyrinthitis, meningitis, and speech and language delays in children. Early treatment prevents all of these outcomes.
How to Prevent Ear Infections: 7 Evidence-Based Strategies
1. Vaccinate — The Most Powerful Tool Available
The pneumococcal conjugate vaccine (PCV15 or PCV20 as of current CDC recommendations) protects against Streptococcus pneumoniae — the leading bacterial cause of ear infections. The annual influenza vaccine reduces influenza-related ear infections. Research shows vaccinated children have significantly fewer ear infections and less antibiotic use compared to unvaccinated peers.
2. Breastfeed for at Least 6 Months
Breast milk delivers maternal antibodies that prime the infant immune system and specifically reduce susceptibility to otitis media. The AAP recommends exclusive breastfeeding for six months, with continued breastfeeding alongside solids for at least one year. Studies consistently show breastfed infants have fewer and less severe ear infections.
3. Feed Upright — Never Lying Flat
When bottle-fed infants lie flat, milk can pool around the eustachian tube openings and flow backward into the middle ear, seeding infection. Always hold the infant at a 45-degree angle or greater during bottle feeding. Avoid propping a bottle and leaving the infant to self-feed.
4. Eliminate Secondhand Smoke Exposure
Tobacco smoke chemicals inflame the mucosal lining of the eustachian tubes, impairing drainage and significantly increasing ear infection risk. Children exposed to secondhand smoke at home have a 37–48% higher risk of developing recurrent ear infections. A completely smoke-free home and car is one of the highest-impact lifestyle changes parents can make.
5. Practice Rigorous Hand Hygiene
Since respiratory viruses — the primary trigger for ear infections — spread via contaminated hands and surfaces, regular handwashing is a front-line defense. Children should be taught to wash hands before eating, after using the restroom, after blowing their nose, and after touching anyone who is unwell. Alcohol-based hand sanitizer is a practical alternative when soap and water are unavailable.
6. Limit Pacifier Use After 6 Months
Multiple studies have identified prolonged pacifier use — particularly beyond six months — as an independent risk factor for recurrent middle ear infections. The sucking action may affect eustachian tube pressure dynamics. Gradual pacifier weaning by 12 months is widely recommended by pediatricians.
7. Keep Ears Dry After Water Exposure
Swimmer’s ear is almost entirely preventable. After swimming or bathing, tilt each ear toward the shoulder to drain water, and gently dry the outer ear with a clean towel. Fitted earplugs designed for swimming offer additional protection. Avoid inserting Q-tips — they compress wax rather than removing it and damage the protective acid mantle of the ear canal.
Frequently Asked Questions (FAQs)
These questions mirror the most frequently searched queries about ear infections on Google — each answer is structured for featured snippet and People Also Ask (PAA) eligibility.
How do you know if you have an ear infection?
| Key signs of an ear infection: ear pain (especially when lying down), a feeling of fullness or pressure in the ear, muffled hearing, fever, and sometimes fluid draining from the ear. In children, tugging at the ear, unusual fussiness, trouble sleeping, and refusing to eat are important behavioral cues. Only a doctor examining the eardrum with an otoscope can confirm the diagnosis. |
Are ear infections contagious?
| Ear infections are not directly contagious. You cannot give someone your ear infection. However, the cold or flu virus that caused your ear infection is contagious. So while the infection cannot spread ear-to-ear, the underlying pathogen can spread from person to person and may result in an ear infection in someone else. |
Is an ear infection contagious if it is bacterial?
| No. Even bacterial ear infections are not directly transmissible from one ear to another. However, certain bacteria (like Streptococcus pneumoniae) that cause ear infections can spread between people through respiratory contact. The bacteria may cause a cold or respiratory illness in another person, which could — but does not always — lead to a secondary ear infection. |
What does an ear infection look like?
| You cannot see an ear infection from the outside. Internally, an infected eardrum appears red, bulging, and cloudy rather than the normal translucent gray. A doctor can visualize this with an otoscope. Externally, possible signs include redness around the ear opening, visible fluid draining from the ear canal, and tenderness behind the ear. |
How do I get rid of an ear infection?
| To treat an ear infection: (1) For mild cases, use OTC pain relievers, warm compresses, and stay hydrated — most resolve in 2–3 days without antibiotics. (2) For bacterial infections confirmed by a doctor, complete the full prescribed antibiotic course (usually amoxicillin). (3) For swimmer’s ear, antibiotic ear drops are the first-line treatment. (4) Avoid inserting anything into the ear canal. |
How to alleviate ear infection pain?
| To alleviate ear infection pain: take ibuprofen or acetaminophen, apply a warm compress to the outer ear for 15–20 minutes, sleep with your head elevated, stay hydrated, and use a humidifier. For children, ensure weight-appropriate OTC dosing. If pain is severe or lasts more than 48–72 hours, see a doctor. |
What causes ear infections in adults vs. children?
| The underlying causes are the same — upper respiratory infections, bacteria, viruses, and allergies — but children get ear infections far more frequently because their eustachian tubes are shorter, narrower, and more horizontal, making drainage harder. Adults’ better-angled tubes are more efficient at draining fluid, which is why adults experience fewer but still significant ear infections. |
What is the difference between ear discomfort from a cold vs. a true ear infection?
| Ear discomfort during a cold is caused by eustachian tube congestion and pressure changes — it typically resolves as the cold clears. A true ear infection involves bacteria or viruses actively multiplying in the middle ear, producing more intense, persistent ear pain, fever, and sometimes fluid discharge. If ear discomfort from a cold does not improve within 3–4 days or worsens, an actual infection may have developed. |
References and Medical Sources
This article was researched and verified using the following authoritative sources:
• Centers for Disease Control and Prevention (CDC) — Ear Infection Basics | cdc.gov/ear-infection
• Cleveland Clinic — Ear Infection (Otitis Media): Symptoms, Causes & Treatment | my.clevelandclinic.org
• WebMD — Understanding Ear Infections: Basics, Anatomy, and Home Remedies | webmd.com
• Medical News Today — Ear Infections in Adults: Causes, Symptoms, and Treatment (Updated Jan 2024) | medicalnewstoday.com
• KidsHealth by Nemours — Middle Ear Infections (Otitis Media) | kidshealth.org
• UPMC Health Beat — Ear Infections: Causes, Symptoms, and Treatments | upmc.com
• American Academy of Pediatrics (AAP) — Clinical Practice Guideline: Diagnosis and Management of Acute Otitis Media | aap.org
• National Institute on Deafness and Other Communication Disorders (NIDCD) — Ear Infections in Children | nidcd.nih.gov
Medical Disclaimer
This article is intended for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional regarding any medical condition or before starting any treatment. Visit homehealthyremedy.com for more evidence-based health guides.
Natural home remedies, skincare secrets, dental & eye health tips, and real product reviews to help you stay healthy the natural way.